Aujourd'hui, mon chat a décidé de changer sa manière de me réveiller. Il ne s'est pas frotté contre moi, et n'a pas miaulé dans mes oreilles. Il a tout simplement vomi sur moi. Plutôt efficace, je dois dire. VDM
Des petites tourtes au poulet individuelles, très facile à réaliser en avance







This piece was put together with assistance from Randy Kim.
One thing that we’re learning in the Trump era is how extensively government power flows throughout our society, as corporations, universities, and law firms scurry to obey the rules that the new administration is putting forward. A few months ago, I found one of these levers in the form of a fee that doctors must pay when they submit medical bills to Medicare or Medicaid. It’s a classic economic termite, a charge that is relatively small such that consumers don’t notice, but one that fosters a significant amount of money for the monopolist. But in this case, there’s a political twist.
But first, let’s go to the problem itself. In January, a reader sent me a note about a fee paid by her father, a licensed marriage and family therapist. Here’s what she said.
In his practice my dad uses a billing software called SimplePractice and in December they started charging a yearly $20 fee to each clinician. They say this fee is to cover the $18 royalty AMA charges SimplePractice for each clinician who uses the software since the software can use CPT codes, as well as a $2 processing fee.
Sure, enough, I went to SimplePractice’s website, and there it is explaining the annual $20 charge for something called a Current Procedural Terminology (CPT) code. SimplePractice says customers must pay the royalty to the American Medical Association, which “owns the rights to CPT codes and mandates the collection of royalty fees for all clinicians who have access to the codes, regardless of usage.”
Last year, SimplePractice sent out a note to its customers announcing this fee structure, to widespread anger. One therapist noted on Reddit, “I may get hate for this but this is the kind of shit that really makes me want to surrender my license and become a life coach, allowing me to continue helping people but opting out of the racket. I’m so tired of feeling exploited.” Another said, “Like wtf, being in private practice is already hard and expensive enough, these little ass fees add up. I might drop emr and go back to paper.”
CPT codes are a way to explain what a clinician did during an interaction with a patient. For instance, the most common CPT code for psychologists is 90837, which is the number that means the clinician provided an hour of psychotherapy. To get payment, they will submit this code to health insurers, whether private, Medicare, or Medicaid, and everyone involved will know what it means. First developed in 1966 for use with Medicare, the demand for extensive medical documentation is now a serious contributor to physician burnout, as "[f]or every 8 hours of scheduled patient time, ambulatory physicians spend more than 5 hours on the electronic health records."
CPT codes are developed by a panel of 21 medical professionals selected by the AMA Board of Trustees who meet three times a year to solicit input from across the medical industry on the latest medical care to create, revise, remove, and determine the relative value of the codes (these relative value units influence insurance reimbursement rates). Twelve panel members are nominated by national medical specialty societies like the American Academy of Thoracic Surgery, while several seats are occupied by representatives from the health insurance industry.
In other words, the AMA isn’t offering a software product. It just runs this process, keeping a list of codes that map to different medical procedures. You would think it would be free, a standard for everyone to use. But it’s not, and the AMA is able to charge a royalty for the license to use those codes. Every medical software company seems to have CPT codes and royalties built into their workflow.
Other similar systems are public. For instance, there’s the World Health Organization's International Classification of Diseases (ICD) codes, which are used by most other countries for free. ICD and CPT codes are complements, not substitutes. ICD is a list of diagnoses- “this patient has depression” “this patient has a pulmonary embolus” while CPT is a list of procedures “I talked to this patient for 60 min” “I did this surgery on this patient.” Most billing systems require both codes, basically the insurer is saying “what did you do” (CPT) and “why” (ICD)? But only one is copyrighted. To put it differently, this situation is a bit like if Fedex owned and designed the zip code system, and got to charge anyone who used a zip code.
The total amount of money to the AMA is relatively small, at least compared to overall cost in our health care system. It’s roughly $300 million a year to the AMA in royalty payments. That’s not nothing; but the impact is far more significant on the politics of health care. To understand why, it helps to start with the importance of this particular trade association.
The AMA is the “doctor’s lobby,” and it has been a powerful force in American politics since it was founded in 1847. The rich American doctor was a 20th century community leader, or a petty tyrant, whichever you might believe. Americans respected their physicians, and doctors were conservative and locally rooted, able to speak with authority on matters of public health. They generally feared the state, but also feared corporate control.
The AMA, as such, jealously guarded this position, routinely opposing government attempts to provide universal health care through a centralized administrative public apparatus, haranguing Democrats as seeking to foster “socialized medicine.” And it worked. The AMA beat Franklin Delano Roosevelt, it beat Harry Truman, and it beat Bill Clinton. The threat of corporatization was perceived by medical professionals as coming from the left.
But in the last 20 years, this dynamic has changed, because most doctors now work for large corporations. The old days of hanging up a shingle in a solo or even small group practice is gone because it’s no longer possible for an individual to bargain with the giants that manage the reimbursements, hospital systems, and payment arrangements necessary to be a doctor. Curiously, the AMA, which one would think has some interest in opposing the mass corporatization of its membership, doesn’t seem to care. For instance, the AMA only took a stance on private equity two years ago, long after its membership had transitioned from majority independent practitioners to majority corporate employees. And a key reason might be because it doesn’t make its money by serving doctors anymore. It makes it from the CPT code monopoly it uses to extract from doctors.
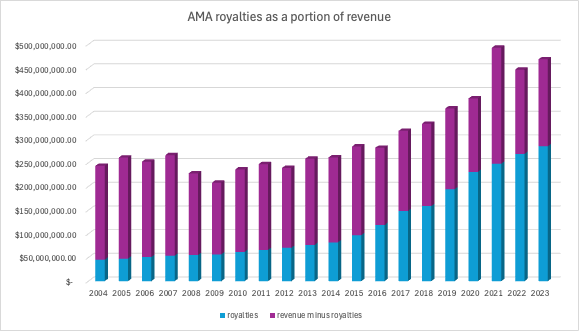
Let’s look at some numbers.
If you look at AMA financial disclosures from 2004 to 2023, you’ll notice three big trends. First of all, dues membership is down. In 2004, it was at $48 million. By 2023, it fell to $33 million. Second of all, revenue is way up, from $243 million to $468 million. And third, there’s an item - “royalties” - that explains it. Royalties, which come largely from CPT code revenue, were about a fifth of the AMA revenue in 2004, at $45 million. In 2023 they were at $308 million, 62% of all revenue, including all the profit, most of the overhead, and the lucrative executive salaries, which have increased by 10x since 2004.
The original CPT codes came out in 1966 to coincide with Medicare, but were published as a book updated annually. It was when electronic medical records took off that the revenue stream picked up.
In 1996, Congress passed the Health Insurance Portability and Accountability Act (HIPAA), which mandated the standardization of electronic health transactions and acted as a catalyst for technology companies to develop software that integrated functions, like standardized medical coding. In 2000, Donna Shalala, the Secretary of Health and Human Services put in a regulation on electronic health records recognizing the AMA CPT codes as the standard for medical billing codes, and did so knowing that it could foster a monopoly and significant price hikes.
In fact, during the rule-making process, according to HHS, “many commenters stated that the Secretary should not recommend proprietary systems as national standards. They believed that the proposed rule lacked a definitive method to guarantee public access to the proposed standards at low cost, and recommended that the government should develop or maintain the national standards or acquire the rights to the standards of choice.” HHS officials responded by noting they had spoken with the AMA about the problem, and that they might change standards if there weren’t “efficient, low-cost distribution mechanisms.”
But since then, prices seem to have gone up, though the pricing itself is opaque. In 2023, the AMA noted that it had a revenue bump of $13.4 million, “as the market for electronic use of digital coding products continues to expand. A three percent price increase, after no increases in the pandemic years, as well as phasing in previous pricing model changes, were also factors." And that copyright is guarded jealously by the AMA. According to a 2011 Forbes article, the AMA even sued “web sites and others to prohibit them from posting comparisons of doctor and other medical fees on the Internet using the CPT code.”
This situation isn’t just a case of unfair rent extraction, though it is certainly that. It’s also a case of political capture of the AMA. At any point, the Secretary of HHS could choose to revisit its standardization on top of CPT codes, and either foster an alternative, allow competition, or demand that the AMA cut prices. There are alternatives. There are ICD codes. There’s also something called SNOMED, which stands for the Systematized Nomenclature of Medicine – Clinical Terms, which is paid for by at a national level. It’s much cheaper than the CPT codes; Japan, for instance, pays less than $1 million. Switching over to a new system, or even allowing a new system would take a lot of effort. A much simpler change would be Congress passing a law invalidating copyrights for public medial standards, such as CPT codes. It’s ridiculous that a public standard on which everyone must operate is subject to extractive royalty payments. The government has a lot of power here, and could actually start to exert it.
And I’m guessing that’s something the leadership of the AMA is keenly aware of. The current CEO of the AMA, James L. Madara, makes $2.5 million a year, and was partners with former Bush HHS chief Mike Leavitt. More than that, he uses the AMA as a platform for other ventures.
He also serves as chairman of Health2047 Inc., the wholly-owned innovation subsidiary of the AMA, created to overcome systemic dysfunction in U.S. health care and located in Silicon Valley. Working closely with the AMA, Health2047 finds, forms and scales transformative health care spinout companies in four fields: chronic care, data utility, radical productivity and health care value. Several companies have been launched to date.
It sure looks like the AMA has turned itself from a voice of doctors into a Silicon Valley tech incubator financed with money extracted from doctors at the behest of the government. That’s a very odd position to be in. If the organizational finances and position of the AMA are dependent on never getting crosswise with the Secretary of Health and Human Services, what does that mean for public health? Moreover, the changes go in both directions. Just as the AMA has become more responsive to political elites than its members, its members have become less invested in the AMA. One consequence of the corporatization of medicine the AMA has ignored is that physicians, realizing they are merely “labor,” and beginning to unionize, formed institutional bargaining systems outside the professional association realm.
And that brings me to two final observations about this particular economic termite. The first is that these kinds of economic termites - basic public information systems that are turned into intellectual property - are pervasive in health care. Just in the pharmacy space, there’s First Databank, Medi-Span, NCPDP, and SureScripts. For my original source, the therapist, there’s a whole host of small but important termites, from email and conference systems that are HIPAA-compliant to special marketing and liability costs. My source sent me a full list, which I edited and put after this essay. If you look it over, you’ll see why therapists - and medical professionals in general - are increasingly opting to work in large corporate practices or only serve the wealthy. They increasingly have no time to do anything but administrative work if operate on their own.
And the second observation is political. One of the more interesting dynamics that I’ve seen of late is how health care lobbyists responded to the appointment of Robert Kennedy Jr, the Secretary of Health and Human Services with a track record of skepticism towards the medical establishment, and opposition to vaccines. Notably, they didn’t really respond, at all.
Before his confirmation hearing, RFK Jr was thinking of attacking the lucrative AMA revenue stream. As the Financial Times reported, “Kennedy’s team has discussed how the CPT process could be done in-house by the Centers for Medicare and Medicaid Services, according to three people briefed on the matter.”
That would be an existential threat to the AMA monopoly. So what was their response a few months later during his confirmation hearing? Here’s Politico, in February.
Kennedy has suggested that hospitals, doctors and drugmakers work together to keep Americans sick, argued that industry influence needs to be ripped away from federal policymaking, insinuated that health institutions intentionally bury inconvenient evidence and proposed lopping off entire parts of the health regulatory structure.
And yet, the country’s most prominent professional society for doctors, the American Medical Association, has not taken a stance on Kennedy’s nomination.

And this decision mattered.
“I believe that silence is consent,” said Thom Tillis (R-N.C.) after agreeing to send Kennedy’s nomination to the floor in a Senate Finance Committee vote last week. “The fact that they haven’t [opposed Kennedy publicly] suggests to me that folks that I’m instructed by are OK with this nomination.”
Was there some kind of deal? Or was the AMA keeping silent in hopes that RFK Jr wouldn’t actually be that mean to them if they played ball? Or were they just paralyzed with fear? That’s not clear, though my guess is that they just didn’t think it was worth it to raise objections.
There are two kinds of populist approaches to health care. One is that exhibited by Bernie Sanders, who thinks that medicine is too expensive and unavailable. And the second is that of RFK Jr, who, to oversimplify, seems to think that expensive medicine itself is often a ruse by large corporations to keep Americans on an unhealthy sugar-and-seed-oil diet. Whether RFK Jr. is right or wrong is a less interesting question than why most of the powerful lobbyists in D.C. didn’t oppose him.
I think the answer to that has to do with fear of what the Secretary of HHS could do to their revenue stream. Whatever you think about RFK Jr, or any cabinet member, it should concern us that the AMA has fewer financial incentives to act as the “doctor’s lobby,” and more incentives to serve as the voice of monopoly.
Thanks for reading!
And please send me tips on weird monopolies, stories I’ve missed, or comments by clicking on the title of this newsletter. And if you liked this issue of BIG, you can sign up here for more issues, a newsletter on how to restore fair commerce, innovation and democracy. And consider becoming a paying subscriber to support this work, or if you are a paying subscriber, giving a gift subscription to a friend, colleague, or family member.
cheers,
Matt Stoller
P.S. Below are eleven extra costs for a therapist. You’ll see plenty of economic termites in there. It’s like this for most industries run by professionals.
Costs to Operate as a Therapist
1. Liability Insurance: From what I understand, this cost has gone up faster than inflation.
2. American Association of Marriage and Family Therapists Membership: Those who buy this member get a discount on liability insurance, but said membership keeps going up while they haven't advocated well for therapists.3. Email - Gmail and the like are not compliant with the Health Insurance Portability and Accountability Act of 1996 (HIPAA). Additional email services are required.
4. Electronic Health Records Software - A HIPAA-compliant way of managing client records, notes, and other information such as SimplePractice5. Teleconferencing - Therapists must use a HIPAA-compliant platform like Doxy or certain Zoom paid plans and if the therapist is EMDR certified there are separate special platforms for that
6. Directory Listings - Psychology Today is the main platform used by consumers to search for a therapist. A profile costs $29.95 a month.
7. State Licensure - Therapists have to meet state licensure requirements which can include things like passing knowledge and ethics tests and completing practicum under a licensed therapist--all steps that cost quite a bit. Once licensed, they pay a recurring fee to the states in which they are licensed to keep them active.
8. Reciprocity - Therapists can only serve clients in states where they are licensed. This has been particularly hard to navigate in the world of online therapy or when a client moves and wants to continue treatment. To create a "solution" for this growing problem, the Counseling Compact Commission (https://counselingcompact.org/faq/) was formed. They are supposed to oversee "a contract among states, allowing professional counselors licensed and residing in a compact member state to practice in other compact member states without need for multiple licenses," but instead of charging one fee to join the compact, they are requiring counselors to pay an administrative fee and state fee for each state they wish to practice in. They also are only allowing licensed professional counselors to use the compact and not Licensed Marriage and Family Therapists. This predicament is not unique to therapists. I know doctors have the Interstate Medical Licensure Compact which is a way for doctors to complete one application and receive multiple licenses, but they too have to pay for the cost of the licenses in any state they want to practice plus $700 to the compact itself.
9. Continuing Education Credits - Therapists are required to get a certain number of continuing education credits each year to keep their license. These can range from a few hundred dollars a year to thousands.
10. Insurance billing - This is so expensive and cumbersome that many therapists forgo insurance altogether and opt for clients to pay out of pocket. If a therapist doesn't provide a decent sliding scale, many low income patients are priced out.
11. State Business License: Therapists can only spend 20-25 hours a week with clients to leave enough time for billing, bookkeeping, marketing, client file management, etc. When therapists start out and are trying to build their client base, they have all of the costs but much lower revenue. It's easy to see how ever increasing operating costs make it very hard for therapists to serve low income patients.


Aujourd'hui, dernier jour de vacances à la montagne. Ne me sentant pas en grande forme, je n'ai pas skié de la semaine pour ne pas me blesser. C'était sans compter la descente en luge familiale proposée par mon mari, 1,5km, qui m'a value une double entorse du genou. VDM
Next Page of Stories